Dynamic Classification of Abnormal Spinal Curves



Adolescent Idiopathic Scoliosis (AIS) is a 3D deformation of the spine. AIS usually affects the younger population in the early stages of puberty and is more frequent in females than in males. As in any other medical condition, assessment is an important step to provide adequate treatment and follow-up for each patient. The Lenke classification is the common criterion used by clinicians to categorize spinal curvatures based on 2D measurements. These are obtained from radiographs of the spine in a standing position. The goal of this study is to classify scoliotic curves. We propose a technique called leave-n-out angle to describe spines from 3D reconstructions, and a Dynamic Ensemble Selection (DES), a Machine Learning method to automatically assess curvature types. Keywords: spine classification, descriptors of the spine, Adolescent Idiopathic Scoliosis, Dynamic Ensemble Selection, machine learning
Adolescent Idiopathic Scoliosis (AIS) is a spinal deformity [1,2]. The AIS causes the spine to look like an “S” or a “C”. AIS affects between 1% and 3% of the population, and it is predominant in adolescents between 10 and 18 years of age, mainly in females. Some serious cases (1 out of 1000) will require surgical treatment. The deformation is usually evaluated through X-rays from the back and side in a standing position. In clinical practice, to assess and treat the severity of the deformation, clinicians use a measurement called the Cobb angle (see Figure 1). This is calculated by finding the most tilted vertebra at the top and at the bottom of the spinal curve. Based on the severity of the curvature, spines can be classified into 6 types of deformation using the widely known Lenke classification method [3].
Although the Cobb angle and the Lenke classification are the primary strategies used to define and treat scoliosis, they do not describe the spine in 3D space. Two spines may look similar on X-rays, but different when viewed in 3D space [4]. Hence, 3D analysis of the spine is critical in understanding and describing the deformity. In this study, we propose a new technique called leave-n-out angles to describe spinal deformations from 3D reconstructions, as well as an automated classification method to assess spinal deformities.
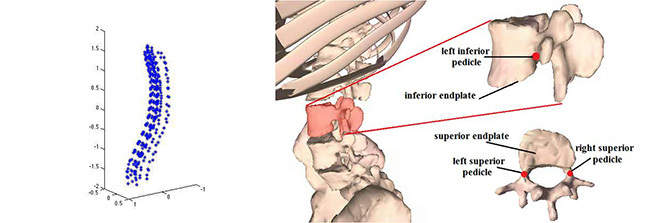
We collected and analyzed 3D spine models of patients with AIS, provided by the Sainte-Justine University Hospital Center. A total of 17 vertebrae are included in each of the 3D spine models, which were reconstructed from X-rays (see Figure 2a). From each vertebra, six landmarks were identified: superior and inferior endplates, left and right superior pedicles, and left and right inferior pedicles (see Figure 2b).
To classify types of curvatures, we need descriptors to depict the shape of the spine (see Figure 3a). Knowing that the spine is a sequence of vertebrae, and assuming that similar spinal curvatures would share similar angles, we proposed the leave-n-out angles technique to describe the spine. It consists of automatically calculating the angle of one vertebra against adjacent vertebrae. Figures 3b and 3c show two examples of this technique. The spine is represented by a line running through the center of 5 adjoining vertebrae, T1 to T5. In example b), the leave-0-out angles show our calculations on the angles of all the adjoining vertebrae T1-T2, T2-T3, and T3-T4. In example c), using leave-1-out angles, we skipped one vertebra in between and calculated the angles of T1-T3 and T2-T4.
In a healthy spine, all the angles have similar magnitudes. Conversely, a spine with scoliosis shows more variation in angle magnitude (see Figure 3a). By varying n in the leave-n-out angles, we could describe the link between vertebrae.

This method is called Dynamic Ensemble Selection because it is based on a set of predictors to categorize a sample. Each classifier was trained with different descriptors of the spine to determine the sample’s category. Depending on each case, the method automatically determines, from a set of predictors, which are the most suited to categorize complex samples.
As an example, imagine a set of trained experts (predictors) responsible for evaluating the spines of new patients. Those 5 experts learned to classify the spine based on different measurements that characterize it (descriptors). Their leader expert (DES) devised a way to use the experts’ knowledge to classify the spines in one Lenke classification type. Figure 4 presents two cases to classify a spine. In case A, when the leader expert asks about the classification of one spine, every specialist agrees on the type, and the spine is classified as 1. Case B is more complex, and the experts do not agree. Consequently, the leader expert decides to use two previous similar cases, knowing their Lenke type. When he asks how these older cases were classified, he realizes that specialists A, B and E classified them correctly, so he uses their opinion to classify the case.

We generated 8 different descriptors of the spine, 3 of them obtained by using the leave-n-out angles technique. Another 3 descriptors correspond to the standard coordinate values in each plane, and the last two are based on the rate of change of the points that form the centerline of the spine [5]. In addition, we applied the DES to perform an automatic categorization of the spines. We train one Random Forest [6] predictor per descriptor, and these predictors act as the specialists in the example above. With our approach, we were able to outperform other ensemble methods to classify spinal deformities.
Our main contribution is the leave-n-out technique to identify the relation between each vertebra with the adjacent vertebrae. Also, we proposed the Dynamic Ensemble Selection as an approach to classify spine deformities automatically. DES offers the versatility of using an ensemble of predictors to categorize one sample. It can even select the set of predictors that is the most likely to classify difficult cases, based on how well they recognize similar cases of a known type. This approach could help clinicians improve the classification of spinal deformities.
For information on this research, please refer to the following paper
E García-Cano, F. Arámbula Cosío, L. Duong, C. Bellefleur, M. Roy-Beaudry, J. Joncas, S. Parent, H. Labelle, Dynamic ensemble selection of learner-descriptor classifiers to assess curve types in adolescent idiopathic scoliosis, Med. Biol. Eng. Comput. (2018) 1–11. doi:10.1007/s11517-018-1853-9.


